


At Least 4762 (9.7%) Missing Nurses Because of the STILL ON-GOING Covid-19 Vaccine Mandates for BC Healthcare Workers
Resulting from Bonnie Henry’s PHO, BC is missing 7% of the nurses that it should have in 2022

Real Numbers Don’t Lie, But Public Officials Did and Still Do
My specialty is in detection of financial reporting fraud and deceptive mechanism. I think and process information like a prudent investor does. I have my own religion and it’s not scientism. Data speaks for itself, and truth doesn’t need to be protected by censorship. The government actions got my full attention in Summer 2021 when I read a strong red flag in Canadian obituary data and government officials were acting irrationally causing immediate damages to public trust.
At least 20% of the public doesn’t want to have anything to do with these covid-19 vaccines. Why would BC health care workers be abnormally more compliant than the public of which they are part of? Several other jurisdictions didn’t implement mandates or quickly backed out of them as they realized that they would have to terminate too many workers and cause public harm.
Historically, up until 2012, the influenza immunization coverage for staff in acute care facilities was no more than 40%, then in 2013, the BC government introduced a coercive vaccinate-or-mask influenza policy which immediately increased the influenza immunization coverage in the mid-70% range, staff became habituated to this policy up until 2020. Then in 2022, the influenza immunization coverage plummeted to 60%.[1]
Obviously, in acute settings, healthcare workers are not sold at all to the necessity of influenza vaccines; Why would healthcare workers change their mind for an experimental covid-19 vaccine? All-cause mortality in 2020 diverges with the public messaging that we were in a deadly pandemic, and in 2021 healthcare workers in hospitals are starting to see weird stuff happening with the rollout of the covid-19 vaccines. I always doubted the covid-19 vaccination rates that BC public officials touted.
At a press conference[2], on Nov 1st, 2021, Health Minister Adrian Dix deceived the public by significantly understating the number of terminated health care workers for non-compliance with coercive covid-19 vaccination mandates. Of the 127448 heath care workers, Dix said that 122059 (95.8%) were fully vaccinated, implying that only 5389 (4.2%) were unvaccinated; Dix reported various unvaccination rates between 2% to 5% for various groups of health care workers. Based on BCNU membership changes in 2022, Dix statements are flat out unrealistic. I believe the unvaccination rate is at least 10%.
In the past few days, I revisited BCNU’s (British Columbia Nurses Union) annual reports for 2022[3], 2021[4], 2019[5] and extracted the following member seniority statistics describing BCNU’s nurse membership base. BCNU counts a member when they paid union dues in the preceding 3 months; thus, nurses terminated in Nov 2021 are still counted in the 2021 totals. It’s in 2022 that the PHO terminated nurses drop out of the membership count. The effect of the PHO is shown in the 2022 member counts.
BCNU’s membership seniority data shows that:
1 – The total membership base of BCNU decreased by a net 2731 or (5.6%) in 2022 from 2021. According to CIHI (Canadian Institute of Health Information) Nursing in Canada, 2021 – Data Tables[6], this is a strong reversal from the preceding nine years of steady growth in the BC nursing supply which averaged a yearly growth rate of 2%.
2 – In 2022, BC lost an absolute massive number of young nurses with 10 years of seniority.
3 – In 2022, there’s a yearly increase in veteran nurses, 15+ years of seniority, a smaller membership base.
4 - There’s a clear divide at the 10 years mark of seniority in terms of year-over-year percentage change.
To bring clarity, I combined below the above six seniority ranges into “<10 years” (young nurses) and “10+ years” (veteran nurses) tranches.
Together, the BC Government and BCNU are obviously aware of that nursing workforce age phenomena because on April 27th, 2023, BCNU came up with a new collective agreement[7] that, by BCNU’s own admission, favors nurses with 10+ years of experience. The aging of the nursing workforce is by design. Here’s the excerpt: “In addition to the general wage increase, the collective agreement includes a significant wage schedule redesign that provides meaningful wage gains including new increment steps at years 10, 15, 20, 25 and 30. There are also significant increases to shift premiums, on-call rates, responsibility pay and isolation travel allowance.”
1. Comparing the 2019 and 2021 BCNU membership levels, the BC nurse’s workforce was growing. The younger nurses were quickly overtaking the veteran nurses who are retiring rapidly.
2. The % of membership of each seniority tranche for 2021 and 2022 show a rapidly aging workforce: young nurses’ proportion of membership drops to 63.3% from 69.5% and veteran nurses’ proportion of membership increases from 30.5% to 36.7% in 2022.
3. Before the Nov 2021 PHO, the nursing workforce was getting younger, and after the PHO it aged rapidly. Following the Nov 2021 PHO, there’s a workforce age composition trend reversal in 2022 vs. 2021.
4. In 2022, young nurses, which represent the bulk of the nursing workforce disproportionately left, or most likely were terminated by the PHO, whereas the veteran nurses increased significantly but from a much smaller base. The 10+ years of seniority tranche is smaller but increased significantly. These are retired nurses coming back to work and out-of-province experienced nurses moving in for higher wages. From the CIHI Data[8], at least 1620 nurses came back from retirement in 2021. Assuming they are still working in 2022, they are part of the the 2031 increase of veteran nurses in 2022. The increase of veteran nurses is mostly attributable to “return-to-practice” nurses. This is not sustainable.
5. In 2022, the net loss of nurses of -2731 (-5.6%) is composed of a loss of -4762 (-9.7%) young nurses offset by a gain of 2031 (4.1%) veteran nurses. Percentages are based on 2021, pre-PHO, BCNU total membership.
The BC government, using coercive mandates, effected a massive workforce reduction of their unionized workers. The latest BCNU collective agreement contributes to an aging workforce and doesn’t address the root causes of nurse shortages. Favoring veteran nurses brings experience but also significantly increases staffing costs and staff turnover because the veteran nurse will retire sooner than the younger nurse. Trying to meet the nursing needs with “return-to-work” nurses is not sustainable. This is something you would never see in the private sector; managers would get fired for that.
Why not favoring higher wages for newly graduated nurses with zero years of seniority to encourage entry into the profession? Not possible because the PHO Covid-19 vaccination mandate discourages entry into the profession. Nurses are 90%+ women. Young nurses wanting to have children have witnessed that Covid-19 vaccination is damaging to fertility and pregnancies. Nurses start leaving the profession after 10 years because they are burning out, exhausted, and work overtime which limits family time.
The BC Government strategy to address the nurse staffing challenge amounts to:
1. remaining recklessly determined on its covid-19 vaccine quackery at-all-costs and irrespective of any other reasonable courses of action that all other provinces have embraced.
2. The BC government realized that young nurses are much less likely to comply with vaccine quackery, and it’s forced to meet its staffing needs with veteran nurses.
3. Attract nurses from other provinces. The recent BCNU collective agreement makes BC nurses the highest paid nurses in Canada and eclipses the second highest paying province, Alberta, by 6% to 20%[9]. BC has effectively declared a nurse poaching war against all other provinces.
4. For BC taxpayers the relative premium that BC is now paying for nurses is in the order of $300M to $400M per year. Imagine a fast ferry scandal each year that the BC taxpayer has to swallow. This goes into the damage bucket caused by the PHO.
5. Veteran and out-of-province nurses are not interested in remote regions, they settle in Vancouver metro. You’ll see that in the section below when you look at the only 3 out of 16 region that didn’t experience a critical loss of nurses.
Bonnie Henry’s April 6th 2023 PHO[10] (Public Health Order) preventing all unvaccinated health care workers to work is still on-going and is in perpetuity, it has no expiry[11]. That’s causing a significant shortage of staff culminating in cancelled surgeries and other health care services. Public health officials claim that staff shortages pre-date the pandemic, that’s a half misleading truth, the PHO has made the situation significantly worse. Pure abuse of power.
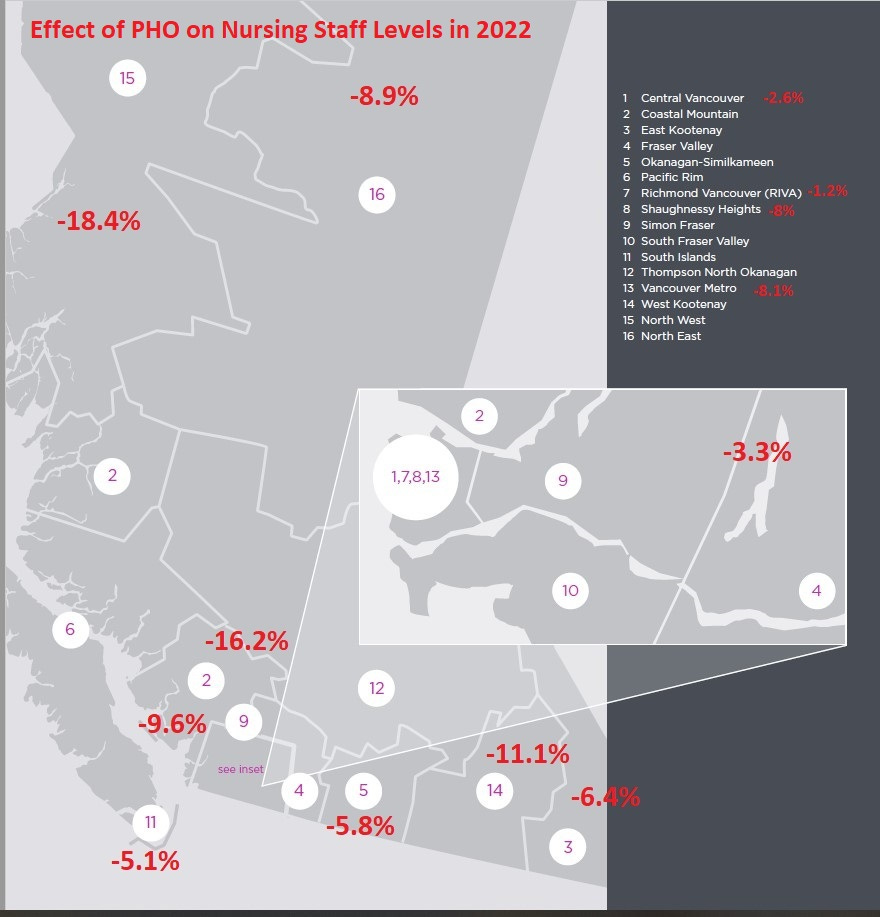
The Geography of the Impact of the PHO (Public Health Order) on BC
BCNU’s annual reports for 2019 and 2022 have granular data of where their members are distributed in 16 regions of BC. 2022 membership data contains the effect of the massive nurse’s termination caused by the PHO and 2019 is the latest pre-PHO regional membership data that I could find from the same source, BCNU. The following map of the 16 regions shows the net percentage change in BCNU members per region between 2019 (pre-PHO) and 2022 (post-PHO). Since BCNU’s 2019 membership level is lower than 2021, the actual percentage change or losses of nurses per region is slightly worse than what the following map shows. Numbers below are slight understatements from 2021.
The following data shows the number of nurses in 2019 and 2022 per region.
Observations:
1. In 2022, BCNU lost 2117 members or 4.4% from 2019 levels.
2. In 2022, 13 of the 16 BCNU regions have fewer nurses than in 2019; This means that anywhere you go outside of the South Fraser Valley, Simon Fraser and Pacific Rim regions, you’ll encounter a more crippled health care system.
Regional Steward and Worksite Data Show BCNU Has Partially Lost Its Ability to Represent Its Members
The BCNU regional membership data also contained stewards and worksites statistics.
Observations:
1. In 2022, BCNU lost 35.5% of its stewards. In 2019, BCNU had 794 stewards, on average 1.04 steward per worksite, in 2022 it had 512 stewards, 0.68 steward per worksite. Stewards are no longer standing with BCNU and have quit in large numbers.
2. In 2022, there are 90.7 union members per steward vs. 61.2 in 2019: That’s a 48% increase in only 3 years. Obviously BCNU stewards are having a harder time fulfilling their duties.
3. The region that has the fewest stewards per member is the South Islands (Victoria) with 0.38 steward per worksite, 142 members per steward.
4. In 2022, while BC general population keeps increasing, there are 0.9% fewer worksites than in 2019. It looks like the PHO is also causing worksites to close.
Read this May 2023 BCNU post: Vice President's Report: "Stewards are the Backbone of our Union", then look again at the stewards statistics above. Is BCNU a crippled union with a broken backbone?
When BCNU was still acting like a union, way back in 2016, 2018, 2014, it used to post things like:
· 2016: BCNU advising members to comply with coercive seasonal flu shot policy: “Members are being reminded to comply with controversial flu shot policy, despite its punitive nature and legitimate efficacy concerns”, “If you have an adverse reaction from a flu vaccine or from wearing a mask, complete an incident report and make a claim with WorkSafeBC.”
· 2018: BC Health Authorities Continue Non-Science-Based "Vaccinate-or-Mask" Flu Policies: “BC health authorities continue to enforce their "vaccinate-or-mask" influenza policy even though Ontario Arbitrator William Kaplan ruled that similar Ontario policies are "insufficient, inadequate and completely unpersuasive."
· 2014: “BCNU believes that … nurses and other healthcare workers should have the right to decide whether to be vaccinated against influenza, based on their understanding of the current evidence and in discussion with their own family physician or other care provider”[12]
The immediate conclusion from the raw numbers is that BCNU has partially lost its ability to represent its members. The nurses of worksites without a steward, as a self-standing group sharing a community of interest, now have a solid reason to file with the BC Labour Board an application for partial decertification and leave BCNU. See: Cancelling a union’s bargaining rights. They only need 45% of the group sharing a community of interest. After decertification, the nurses will have regained their individual bargaining rights and can choose a course of action that will force the results that their conscience demand.
There’s more to it and its beyond the scope of this article. But here’s a teaser: The BC government has been contributing 1% of nurses’ aggregate wages to BCNU’s Retiree Benefit Fund (RBF) since 2008. For example: $35.19M and $32.02M in 2022 and 2021 were contributed by the BC government to BCNU’s RBF. From these two numbers we can infer that the nurses’ payroll increased by 10% while the nurse staffing level decreased by 5.6%. That’s one effect of Bonnie Henry’s PHO.
On the 2022 financial statements of BCNU, the RBF now represents $424M, or 74% BCNU’s total assets. BCNU has not dispensed of these public funds as intended, something that Minister Adrian Dix is aware since at least 2018.[13] The RBF generates investment returns that seem to partially accumulate into BCNU’s internal funds via a council motion. Thus, it does appear like that the BC government is financially contributing to BCNU, that would be an “Unfair Labour Practice”[14]. So, if you’re wondering why BCNU appears to fail to represent the terminated nurses, here’s your answer. An eventual determination that an Unfair Labour Practice took place is a bit like a predicate violation for the bigger violation of the “Duty of Fair Representation”[15]. Another aspect of this is that BCNU enjoys a tax-exempt status, yet the bulk of its assets are investments and for the last 5 years, BCNU has been generating consistent excess revenues over expenses (profits). BCNU looks more like an investment management operation masquerading as a failing union. This paves the way for BCNU’s decertification as a union.
It is very important for nurses to realize that BCNU has not only lost its capacity to represent, but it is also a financially captured entity by the BC Government. BCNU should have initiated collective bargaining over the vaccination mandate issue as soon as its last collective agreement lapsed on March 31st, 2022, go on strike, but it didn’t. In that sense, BCNU is now an instrument to enforce dim-witted public health policies that are a public health hazard: The PHO that prevents nurses to go back to work is a condition that endangers, or is likely to endanger, public health. As long as nurses are members of BCNU, they have relinquished their individual bargaining power to a union apparently captured by their employer.
The communist, one-size-fits-all policy of Bonnie Henry is a public health management disaster wreaking havoc throughout BC. That’s what communism does: it applies rules across the board from the narrow perspective of deluded and privileged ideologues. While these bureaucrats signal virtue by signing their emails with acknowledgment of living on First Nations unceded territories, by gutting the nurse’s workforce in the regions they have also removed healthcare services to the First Nations. Pure hypocrisy and typical of communism. There’s nothing inclusive and equitable in Bonnie Henry’s PHO; it’s harming minorities and especially the remote regions of BC.
Monetary Damages
One particular motive for the BC Government to understate the covid-19 vaccination mandate unlawful firing is to make class action lawsuits less appealing. With the new understanding that massive unlawful layoffs took place and with a low-end estimate of at least 4762 nurses or 9.7% of the nursing workforce, we can start estimating the parameters of class action lawsuits.
For example, in the article: “British Columbia: Employer That Engaged In "Hardball Tactics" To Manufacture Just Cause For Termination Must Pay Over $200K In Damages”, the $208K settlement was the sum of $58K of wrongful dismissal (lost pay), $50K of aggravated damages and $100K of punitive damages. Nurses earn on average $100K and above. They’ve been wrongfully terminated for nearly 2 years. Low-end damages per nurse could be in the $300K. Multiply this by 5000 nurses and we get a class action lawsuit for at least $1.5B. This is just for nurses. There are tens of thousands more of BC public servants who have been subjected to the same abuse.
A higher end point estimate comes from this Epoch Times Article: EXCLUSIVE: Canadian Soldier’s Refusal of COVID Vaccination Not a ‘Conduct Deficiency,’ Grievance Committee Rules where a military administrative tribunal ruled that refusing the covid-19 vaccination wasn’t a conduct deficiency. Now, 329 service members are suing for $500M, that’s $1.52M per aggrieved. For 5000 terminated nurses that’s $7.6B, which strangely matches with the real fiscal surplus that BC should have declared in 2022…
Is the BC Government aware that it is acting unlawfully, that it causes public harm? Looking at the totality of the circumstances I say more likely than not, yes.
1. As pointed out above, the BC Government, by the way it structured the new BCNU collective agreement, tacitly admitted that young nurses, the bulk of its nursing workforce were most significantly affected by the mandates.
2. The BC Government knows that there’s a hard ceiling in vaccination rate uptake of about 80%. This is known from the influenza vaccination rates of healthcare workers. That hard ceiling was only achieved by introducing a coercive vaccinate-or-mask policy in 2013, before that, the rate drops below 40%.
3. All other provinces cancelled similar policies as soon as perceived benefits vanished or didn’t even impose them.
4. BC has a long history of financial reporting misstatements: “Four different auditors general over the last eleven years, including this year, have identified a significant misstatement in the financial statements.”[16] - Michael Pickup, BC General Auditor.
5. In 2022, the CBC reported: Auditor general says B.C.'s surplus should have been $6.5B higher. Let’s dig into this a bit more a relate it to the PHO…
When an organization intends to break the law or to act recklessly with moral turpitude, they’ll estimate their liability and create an accounting reserve in case they have to pay up. The CBC reported that, in 2022, the province had a forecasted deficit of $9.7B. Instead, the province declared a surplus of $1.3B and Michael Pickup, BC General Auditor, reported that the surplus should have been $6.48B higher to $7.78B. We are in the presence of a potential economic differential of $17.5B!!! Either the province was incredibly incompetent in its first estimated deficit, or within a year, (as BC committed to unlawfully fired their workforce) it realized that it needed to squirrel away $11B to $17.5B in case they have to pay for damages. Another explanation contributing to this huge differential is the real possibility that BC fired at least 10% of its workforce over the covid-19 vaccination mandates, and realized savings in avoided payroll expenses.
There’s an institutional investment asset class called litigation finance. Litigation finance is when a third-party, invests in a lawsuit for a share of the profits. A legal claim is like an investable asset: It’s worth money, but there’s risk. Litigation finance investors will require at least a 10x return on the non-recourse funding that they provide. The terminated nurses’ minimum damages of $1.3B imply that litigation finance hedge fund funds could be willing to invest $130M in legal fees. That buys you an army of lawyers. The size of the damages is a sweet proposition for hedge funds investing in litigation finance. I think the province is well-aware that it painted multiple litigation finance and class action lawsuit bull’s-eyes on its back.
Conclusions
Based on membership statistics from BCNU’s annual reports, the BC government deceived the public by understating the loss of health care workers. By using low-end estimates, potential personal and economic damages of the PHO are now quantifiable. Large potential damages are class action lawsuit magnets which the BC government has most likely planned for (financial reporting of poor quality)
The drop of 4762 young nurses in 2022 is fully attributable to the PHO. I do not believe that these young nurses retired, burned out, decided to go on maternity leave or choose to abandon their well-paying careers to go work at Walmart.
In 2012, BCNU had 40000 members and in 2021 it had 49177 members. Over nine years, this represents an average annual growth rate of 2% which is very close to the population growth rate and confirmed by the CIHI (Canadian Institute of Health Information) Nursing in Canada, 2021 – Data Tables. Using a 2% annual growth in nurses, the 2022 BCNU membership should have been around 50160 nurses. Instead, because of Bonnie Henry’s PHO coercive and senseless covid-19 vaccination mandate, we have only 46446 BCNU members in 2022, a shortfall of 7% from what BC should have.
The PHO has set back the BC nursing supply by at least 5 years, while the population grows at 2% per year. Bonnie Henry chose to service 10% more population with 5.6% fewer nurses. The PHO also caused damage to the BC health care system by prematurely aging its workforce. There’s no doubt that the PHO has caused tremendous public harm and damages to BC. It will take years to recover from that abuse of power.
Public health officials avoid accountability by saying that staff shortage pre-dated the pandemic, but what they’re not saying is that staffing levels were increasing, now the nursing staffing levels are decreasing because of the PHO. The public loss of trust in public health is not caused by crazy conspiracy theorists, it’s rightly caused by lying public officials who have introduced a public health hazard by crippling the healthcare system.
To all nurses still employed and especially those in rural regions, in order to get your terminated sisters back to work, you need to get out of BCNU and regain your individual bargaining rights by filing for partial decertification. BC Rural Health Care Alliance, a group of at least 37 mayors, is trying to solve their healthcare shortage. Rural mayors should team up with local affluent businesses and people to support union decertification. Once healthcare workers are out of a union and have regained their individual bargaining right, they’ll be able to apply pressure on employers such that unreasonable edicts coming down from the province will become impossible, too expensive and politically toxic. Free from being tied to a union, health care workers in the regions will hold the balance of power because they’ll be able to abort unreasonable one-size-fits-all policies. In the regions, health care workers are in such high demand that they naturally hold the balance of power, they don’t need a union. Labor scarcity will be on their side for a very long time.
Remove the corrupt unions and colleges. Let nurses be nurses, and doctors be doctors, without the interference of lunatic and ideologue bureaucrats. Let the goodwill of healthcare employers and workers solve this. The Government’s role in healthcare should be restricted to paying for it, not managing it.
[1] Final Report Influenza Vaccine Coverage Staff of Acute Care Facilities British Columbia, 2021/22
[2] Vernon Morning Star – Nov 1st, 2021 - 3,300 unvaccinated B.C. health-care workers placed on unpaid leave following mandate
[3] BCNU 2022 Annual Report p.16
[4] BCNU 2021 Annual Report p. 9
[5] BCNU 2019 Annual Report p.14 * 6046 members of unknown seniority were proportionally attributed to 42513 of known seniority tranches. *
[6] CIHI (Canadian Institute of Health Information) Nursing in Canada, 2021 – Data Tables, 4a Supply Tab
[7] April 27th, 2023 – BCNU Members Vote in Favour of New Provincial Collective Agreement
[8] CIHI (Canadian Institute of Health Information) Nursing in Canada, 2021 – Data Tables, 4b Number, return to practice - Supply Tab
[9] Nurse Wage Comparison Charts, CFNU Member Organizations
[10] HOSPITAL AND COMMUNITY (HEALTH CARE AND OTHER SERVICES) COVID-19 VACCINATION STATUS INFORMATION AND PREVENTIVE MEASURES – APRIL 6, 2023
[11] P.22 F. EXPIRATION AND COMPLIANCE - HOSPITAL AND COMMUNITY (HEALTH CARE AND OTHER SERVICES) COVID-19 VACCINATION STATUS INFORMATION AND PREVENTIVE MEASURES – APRIL 6, 2023
[12] BCNU Update Magazine – Dec 2014 – Bah!Flu Bug!. P.14
[13] FOI Request - HTH-2020-04783 – Response Package p.93, 110, 111.
[14] BC Labour Relations Code - Unfair labour practices – section 6(1)
[15] BC Labour Relations Code - Duty of fair representation – section 12
[16] P. 7 - Auditor General’s Report on the Financial Audit Work: Fiscal Year 2021/22
Are there any numbers for missing nurses available for Ontario?